

Female genital mutilation is defined as ‘all procedures that involve partial or total removal of the external female genitalia, or other injury to the female genital organs for non-medical reasons’ (World Health Organization (WHO), 2021). An estimated 200 million women and girls worldwide (UNICEF, 2016) have experienced the physical, psychological, and social sequelae of female genital mutilation, with associated healthcare costs of 1.4 billion US dollars per year (WHO, 2021). In 2011, it was calculated that 137000 women and girls with female genital mutilation resided in England and Wales, (MacFarlane and Dorkenoo, 2015) costing the NHS approximately £100 million annually (Hex et al, 2016).
Female genital mutilation is recognised as a form of gender-based violence and human rights violation rooted in gender inequality (WHO, 2021). It is a global public health concern, presenting an increasing challenge to countries with large diaspora. Despite prevention efforts, the pace of decline is uneven and UNICEF (2022) estimate that an additional 2 million girls could be at risk of female genital mutilation by 2030 as a result of social disruption caused by COVID-19. The practice, which has been illegal in the UK since 1985, is often justified by cultural or religious reasons underpinned by the desire to control female sexuality (Berg and Denison, 2012).
Between 2015 and 2022, more than 80000 women and girls with female genital mutilation accessed NHS services in England (NHS Digital, 2020). Most (80%) were identified through maternity services, suggesting that non-pregnant women are less likely to present (Karlsen et al, 2023). This may be because female genital mutilation specialist clinics in areas of high prevalence tend to be placed in maternity services and rarely cater to non-pregnant women (UNICEF, 2020).
In 2015, a mandatory reporting duty was introduced in England and Wales (only) for healthcare professionals, social workers and teachers to report girls identified with female genital mutilation, under the age of 18 years, to the police (Gov.uk, 2015). The same year, a compulsory female genital mutilation dataset collection was introduced in England (only), requiring healthcare professionals to record attendances of women and girls with female genital mutilation when presenting to acute and mental health trusts and GP surgeries (Rittenberg, 2018; NHS Digital, 2020).
In 2019, NHS England commissioned five clinics specifically for non-pregnant women in areas of high prevalence and gave additional funding to three pre-existing clinics (including the one described in this article) (Hanlon and Hex, 2021). These new clinics were modelled on the midwife-led Acton clinic described in this article (Albert and Wells, 2020).
A study by Gordon et al (2007) presented longitudinal data from a female genital mutilation service in west London for both pregnant and non-pregnant women over a 10-year period, from 1995 to 2005. They saw 767 new cases in this period; performed 215 deinfibulations as day case inpatient surgery, (mostly under spinal or epidural anaesthesia) and reportedly two women complained of psychosexual problems. They recommended that female genital mutilation services should employ a trusted interpreter and expedite access to deinfibulation for newly married and pregnant women. Audits from other female genital mutilation specialist services have subsequently been published (O'Connell et al, 2005; Brown et al, 2013; Gov.uk, 2015a, b; Rittenberg, 2018; Hanlon and Hex, 2021), but these are primarily restricted to annual figures, are for pregnant women only or combine maternity and gynaecology services and were all published prior to significant changes in female genital mutilation legislation in 2015.
This article aims to fill a gap in UK female genital mutilation research regarding care of non-pregnant women with female genital mutilation. To the authors’ knowledge, no other papers have examined longitudinal data from a dedicated non-pregnant women's female genital mutilation specialist service in the context of recent national policy changes and increasing international work to eliminate female genital mutilation. This study explored trends in demographic, clinical and therapeutic variables in one clinic over an 11-year period. The analysis demonstrates how changes in presentation and management have taken place over time and can help to inform future service commissioners. A further article will examine changes to clinical practice.
Methods
A retrospective case note review was conducted of clinic records from 1 October 2008 to 31 December 2019. Information on demographic (year and country of birth, length of time in the UK, level of English spoken), clinical (type of female genital mutilation, details of procedure, concomitant symptoms and intervention received, age when cut, and route of referral to the service) and therapeutic (psychological assessment) variables were retrieved. To set the data in context, the historical development and current structure of the clinic are described.
Study setting and specialist clinic development
In response to a clear unmet need (articulated in a series of community consultations and preceded by closure of a previously well-attended local hospital service (Gordon et al, 2007), the first dedicated community-based clinic for non-pregnant women, the Acton African Well Woman Clinic, was set up in 2007 by a midwife from Imperial College Healthcare NHS Trust and a Somali community health advocate from Ealing Primary Care Trust. A tripartite model integrated a midwife, a health advocate and a trauma counsellor into a holistic woman-centred service. Two specialist midwives, experienced in perineal suturing, were trained to perform simple deinfibulation under local anaesthetic (Table 1). Governance was provided by quarterly steering group meetings consisting of team members, a female genital mutilation survivor, representatives from the local acute NHS Trust, primary care NHS Trust and specialist charity, FORWARD.
Table 1. Clinical definitions for female genital mutilation-related procedures
| Term | Definition |
|---|---|
| Previous or history of type 3 | The current state where a woman originally had type 3 female genital mutilation but has been deinfibulated/opened before presenting at the clinic |
| Deinfibulation | Opening the sealed vulva of a woman with type 3 female genital mutilation to expose the vaginal opening and urinary meatus |
| Simple deinfibulation | Deinfibulation carried out under local anaesthetic, maybe on the same day in hospital outpatients or community setting. There is usually no attempt to expose the clitora glans and/or prepuce. In some countries, this might be carried out by a traditional circumciser on the wedding night or even forcibly by the husband |
| Complex deinfibulation | When type 3 female genital mutilation is accompanied by a cyst, keloid scar or other complex presentation, deinfibulation is carried out by a suitably trained doctor. This may require epidural, spinal or general anaesthesia and be undertaken in theatre as day case surgery. There may be an attempt to expose clitoral tissue |
| Reinfibulation | The procedure to re-close the vulva opening in a woman after she has been deinfibulated (ie after childbirth). This is illegal in the UK |
| Reconstruction | A surgical procedure carried out to restore original genita appearance. Clinics exist in some countries in Europe, Africa and in the USA. Not available in the UK |
In 2017, as a result of funding challenges, the clinic was re-located to gynaecology outpatients at Queen Charlotte's and Chelsea Hospital alongside a pre-existing clinic for pregnant women. The service was renamed the ‘Sunflower Clinic’, in recognition of the fact that female genital mutilation is not solely an African practice.
The clinic model, described in Box 1, was designed to reduce barriers to accessing services for those who had experienced female genital mutilation, providing a culturally sensitive trauma-informed approach to care (Rittenberg, 2018). These principles emphasise establishing trust, ensuring safety and yielding control to the patient, while minimising discomfort, re-traumatisation and shame (this is particularly important when performing genital examinations, as this can elicit flashbacks or vasovagal response (Rittenberg, 2018).
Box 1.Key elements of the specialist clinic model
- All-female team, midwife-led, non-pregnant women only
- Holistic tripartite model of care, integrating and co-locating a counsellor and Somali/Arabic-speaking health advocate into consultations and offering support during deinfibulation
- Easy access: community-based/hospital outpatients, accepting self-referrals, no geographical boundaries, women seen within 2 weeks of making contact
- Offering walk-in same day deinfibulation under local anaesthetic or fast-track deinfibulation under general anaesthetic (within 4–6 weeks)
- Counsellor provides initial psychological assessment and up to 8 weekly one-to-one psychosexual/trauma sessions with flexible extension period if required
- Health advocates provide language and emotional support, engage with local female genital mutilation practising communities, advertise clinic and are bridge between staff and patients
- Link to named gynaecology consultant for complex case referral
Each consultation includes: taking a medical history, a safeguarding assessment, a genital examination to diagnose type, a psychological assessment, discussion about UK law and female genital mutilation as a human rights violation, exploring reasons why the woman believes it was carried out, discussing her right to physical integrity and giving detailed information of the health consequences of female genital mutilation. More detail on this model of care has been described elsewhere (Albert and Wells, 2020).
Key variables were routinely recorded for individual patients to ensure a robust safeguarding assessment, clinical history and record of intervention. From 2015, several new items were added to data collection; for example, questions related to who perpetrated the cutting (to determine whether there was an increasing trend in medicalisation) and whether the woman had spoken to a professional about female genital mutilation before.
Data collection
Relevant data were accessed from the hospital database using a standardised excel spreadsheet, stored in encrypted files and anonymised prior to analysis. As a result of the service relocation, from the original GP-based community venue to the acute trust in 2017, it was not possible to retrieve original records before this date; however a summary of recorded data from this period was used.
Patients did not participate in the writing of this review, however, the steering committee (including those who had experienced female genital mutilation) met regularly and contributed to the ongoing design and development of the service.
Ethical considerations
The study was registered as a clinical audit on the 02/12/2020 (#562) by Imperial College Research Ethics Committee, and an ethics exemption was granted. Informed consent was waived as data were accessed retrospectively and de-identified prior to analysis. The study was carried out in compliance and following the principles outlined in the Declaration of Helsinki.
Results
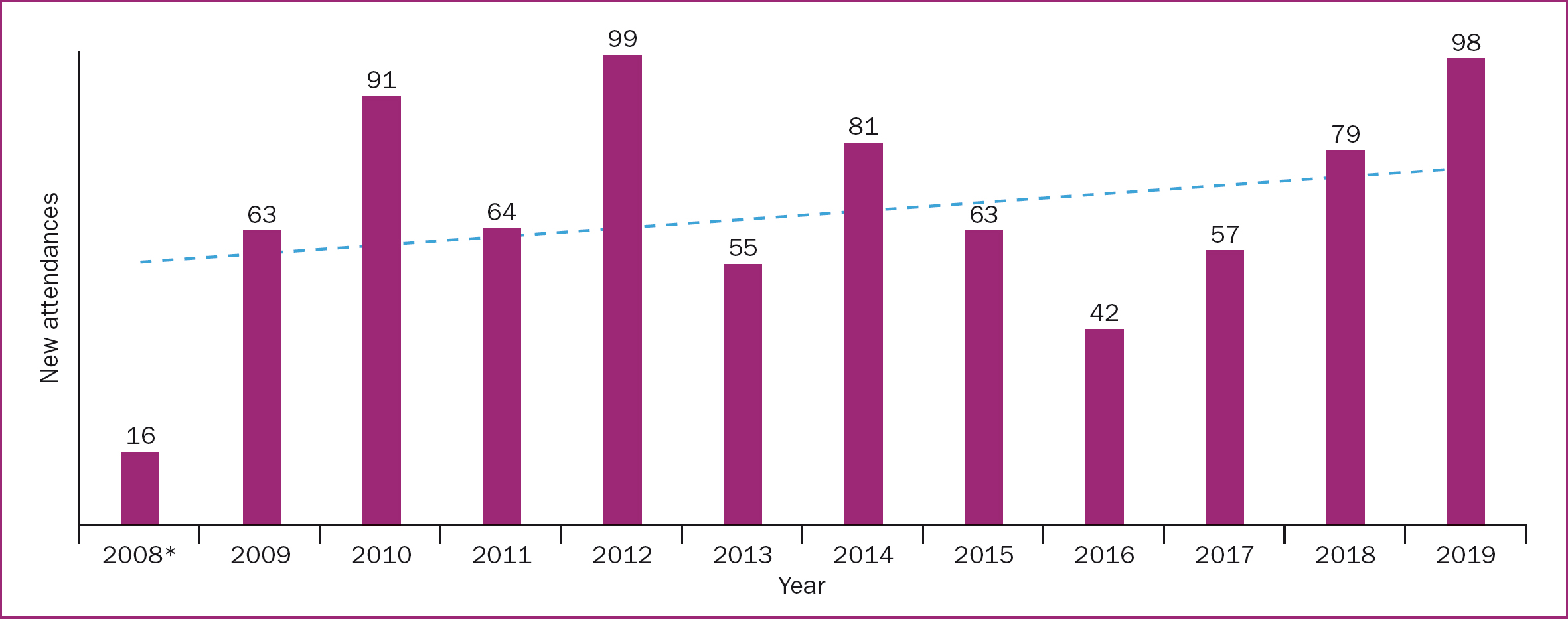
A total of 808 new clients/first consultations were recorded from October 2008 to December 2019. New attendances by year are shown in Figure 1. Including follow up appointments and counselling sessions, there were more than 2000 total attendances over this period.
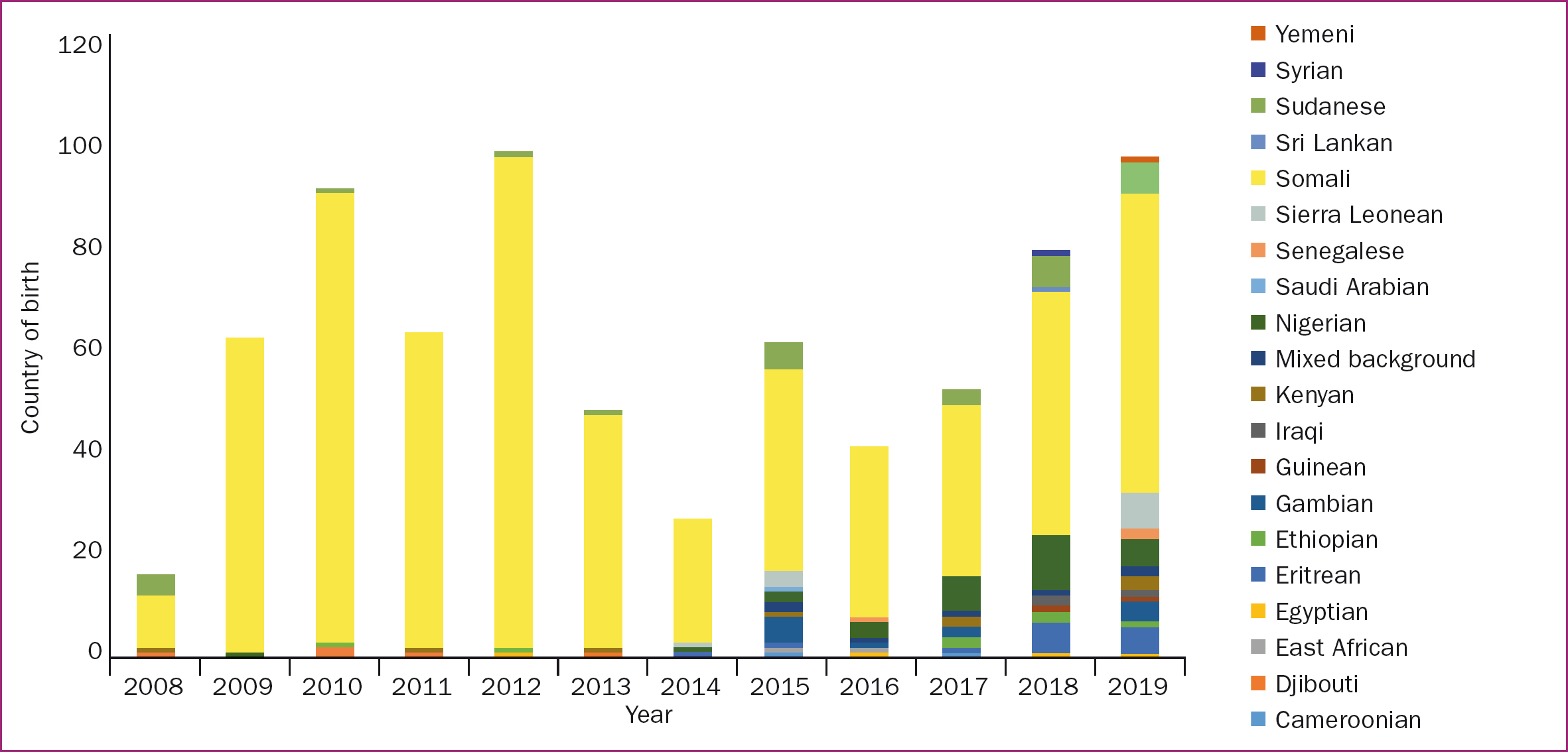
Women's ethnicity (Figure 2) was recorded according to their mother's ethnic background, but there were several examples of mixed ethnicity. In total, 18 ethnic origins were documented. Most women (73.4%) were of Somali background. Before 2015, only 5.4% of attendees were from other ethnic groups (Djibouti, Egyptian, Eritrean, Ethiopian, Gambian, Kenyan, Nigerian, Sierra Leone, Sudanese), while 94.6% were Somali. However, between 2015 and 2019, 36.0% of women were from backgrounds other than Somalia.
More than 90% of women were born in Africa, including one Caucasian woman with type 2 female genital mutilation. The remaining 10% were born in the Middle East (n=5; Iraq, Dubai, United Arab Emirates and Saudi Arabia), Sri Lanka (n=1), the UK (n=4) and Europe (n=5; Spain, Norway, Germany, France, the Netherlands).
Table 2 shows the ages when women experienced female genital mutilation. Almost half (46.7%) were between 5 and <10 years old. Eight were over 18 years old. Several women reported being cut twice, and one woman recalled being cut three times (because she had not been cut ‘enough’ the first time). Several women disclosed that they were already residing in the UK and were taken abroad to be cut. Two women were cut in the UK, both more than 10 years previously. Neither wished to make a police report.
Table 2. Age when experienced female genital mutilation
| Age (years) | Frequency, n=808 (%) |
|---|---|
| <1 | 25 (3.1) |
| 1–5 | 60 (7.4) |
| 5–9 | 377 (46.7) |
| 10–14 | 93 (11.5) |
| 15–17 | 6 (0.7) |
| ≥18 | 8 (1.0) |
| Not cut | 2 (0.2) |
| Don't remember | 55 (6.8) |
| Not recorded | 182 (22.5) |
From 2015 onwards, women were asked who had carried out their cutting. Overall, 122 said that they were cut in their own home by a traditional circumciser without pain relief, and 35 were cut by a healthcare professional. All nine women born in Europe were cut between the ages of 5 and 15 years old.
Table 3 shows women's ages when they accessed the service. The largest proportion (20.2%) were aged 25–29 years old. Four attendees were more than 60 years old. One 17-year-old pregnant woman attended for deinfibulation in 2011 (before introduction of the mandatory reporting duty). Although the clinic was essentially for non-pregnant women, 27 pregnant women self-referred. All were booked at local maternity hospitals. The majority said they were unable to access antenatal deinfibulation at their own hospital. There were also several women with intact type 3 who had previous caesarean sections without being offered deinfibulation.
Table 3. Age when accessed service
| Age (years) | Frequency, n=808 (%) |
|---|---|
| Not recorded | 159 (19.7) |
| Under 18 | 1 (0.1) |
| 18–24 | 147 (18.2) |
| 25–29 | 163 (20.2) |
| 30–34 | 123 (15.2) |
| 35–39 | 107 (13.2) |
| 40–44 | 55 (6.8) |
| 45–49 | 31 (3.8) |
| ≥50 | 22 (2.7) |
A total of 310 (38%) women travelled 8km or less to attend the clinic (Figure 3). Outside London, women travelled from all over the UK. One cohort of women travelled more than 300km (note: Figure 3 does not include 140 women whose place of residence was not recorded, one woman who came from Germany and another who came from Belfast).
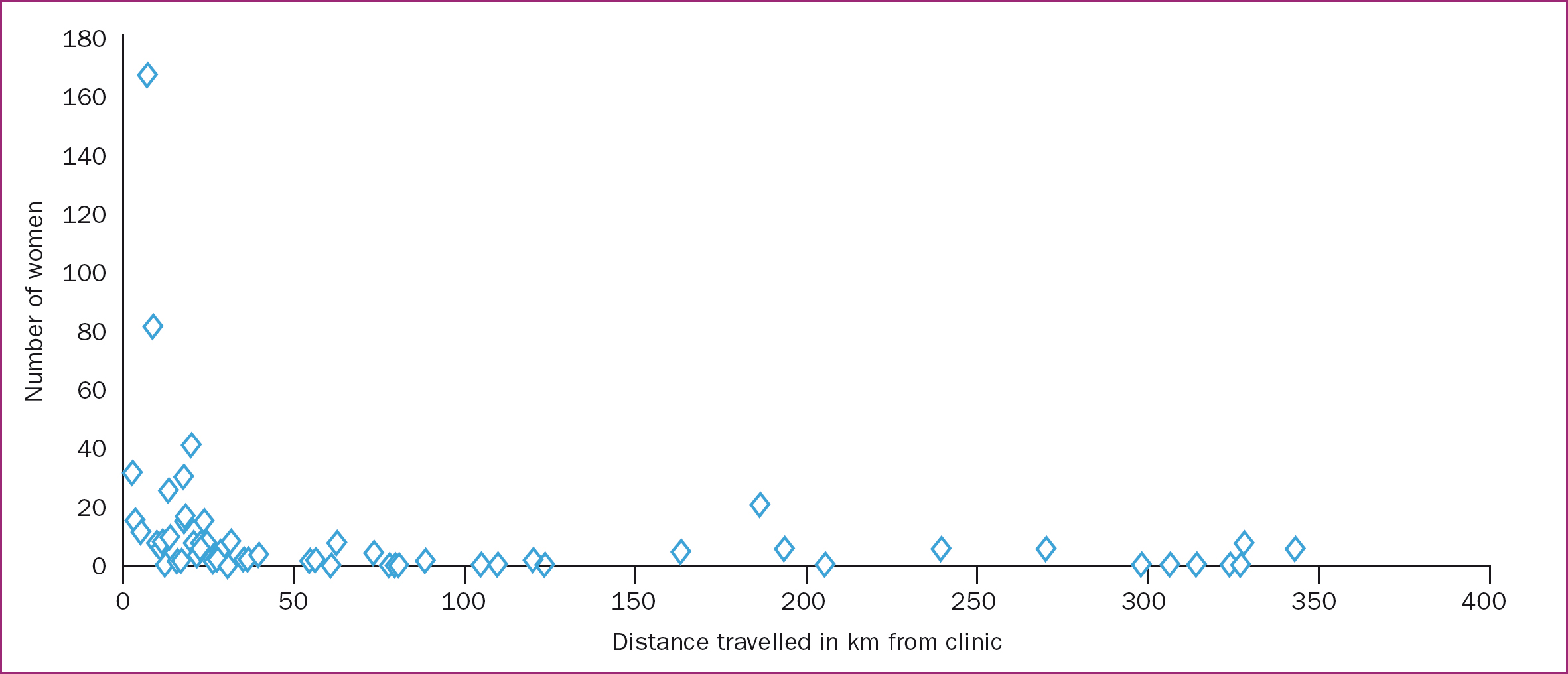
Table 4 shows how long women had been living in the UK. Nearly half (45.4%) had been in the UK for 10 years or fewer, 29.8% for more than 10 years and 21 (2.6%) for over 25 years. A small proportion (2.8%) had only been in the UK for a few months. Many women had lived in other countries ‘en route’ to the UK and had family members dispersed around the world. More than 10% of attendees were healthcare professionals and 5% were refugees/asylum seekers.
Table 4. Length of time living in the UK
| Number of years | Frequency, n=808 (%) |
|---|---|
| <1 | 23 (2.8) |
| 1–5 | 151 (18.7) |
| 6–10 | 193 (23.9) |
| 11–15 | 122 (15.1) |
| 16–20 | 67 (8.3) |
| 21–25 | 31 (3.8) |
| 26–30 | 18 (2.2) |
| ≥30 | 3 (0.4) |
| Born in the UK | 5 (0.6) |
| Not recorded | 195 (24.1) |
Women found out about the service from multiple sources. A series of advertisements on Somali satellite television were shown twice weekly between 2009 and 2012 (until funding ceased). Between March 2009 and December 2010, 375 phone calls were received with subsequent surges in clinic attendances.
The majority of women self-referred by phone call, email, WhatsApp or text, 160 were recommended by friends and/or family, 84 were referred by their GP (often for difficulties taking cervical smear tests), 34 were referred by other healthcare professionals, and 60 said they had searched the internet. Women often mentioned more than one route of referral. Other sources included lawyers, social workers and non-government/charitable organisations. For 258, the method of referral was not recorded. Many women said it had taken years to find help for their female genital mutilation-related symptoms.
From 2015 to 2019, level of English spoken was recorded. Almost 1 in 8 (11.5%) had either basic English or none. Somali and Arabic were the most common first language. Nearly one third (29.8%) said that they had never spoken in detail to a healthcare professional about female genital mutilation before and many women did not want appointment letters sent home or their GPs informed of their consultation.
Clinical variables
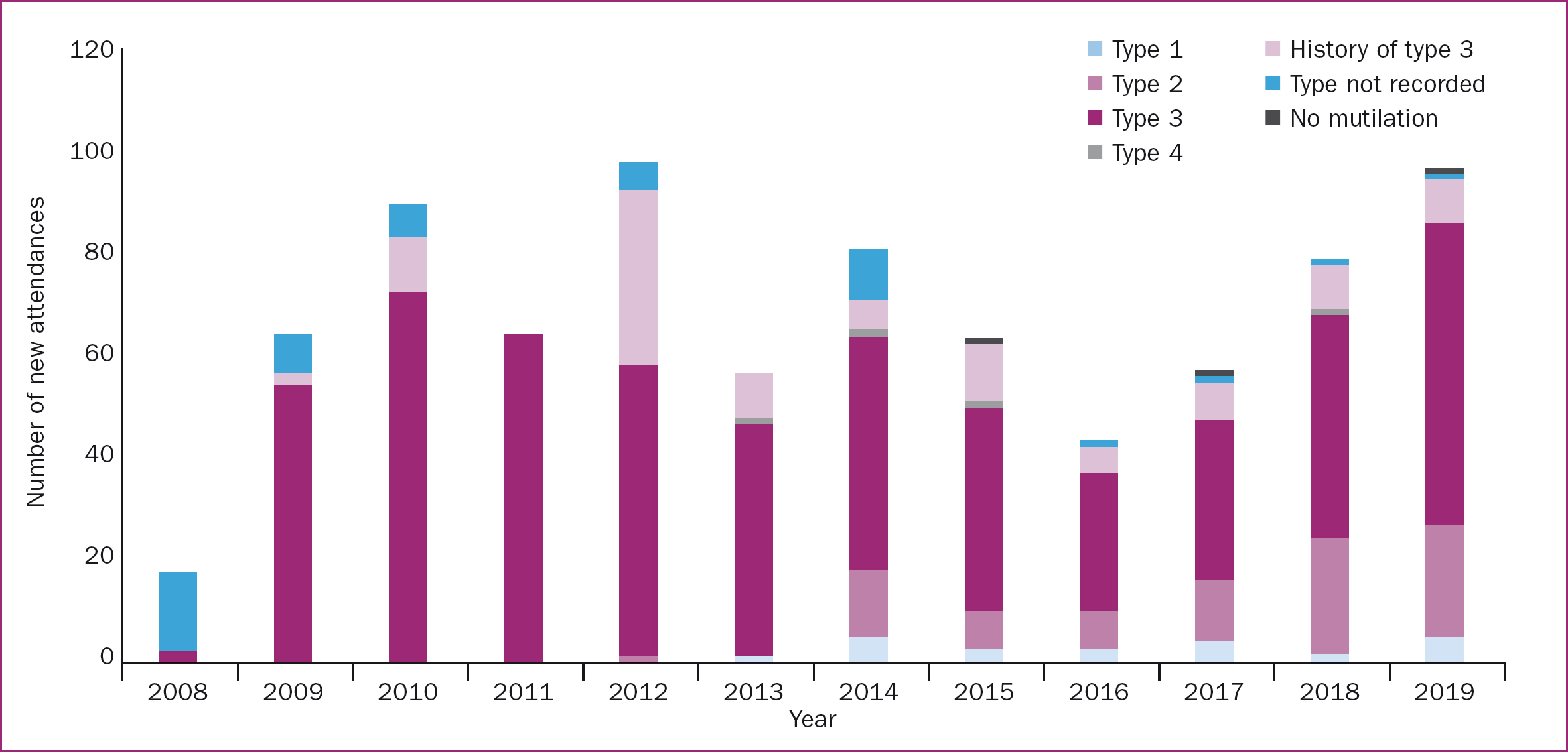
In total, two thirds of women (67.0%) were diagnosed with type 3, 12.9% with a history of/previous type 3, 9.8% with type 2, 3.2% with type 1 and 0.7% with type 4. In 49 cases (6%), no specific type was recorded. Female genital mutilation is classified into four types, depending on the varying levels of genital trauma (Table 5).
Table 5. Classification of female genital mutilation types
| Type | Definition |
|---|---|
| I | Partial or total removal of the clitoral glans and/or the prepuce (clitoridectomy) |
| II | Partial or total removal of the clitoral glans and the labia minora, with or without excision of the labia majora (excision) |
| III or infibulation | Narrowing of the vaginal orifice with creation of a covering seal by cutting and appositioning the labia minora and/or the labia majora, with or without excision of the clitora glans (infibulation) |
| IV | All other harmful procedures to the female genitalia for non-medical purposes, including pricking, piercing, incising, scraping and cauterisation |
Source: World Health Organization (2020)
After 2013, more women presented with type 1 and type 2 female genital mutilation, but there remained a high incidence of women with type 3. Two women did not have female genital mutilation but were seeking proof of this. One was seeking asylum and feared being subjected to female genital mutilation if forced to return to her country of origin. The other had been raped, drugged and beaten as part of ritual abuse and wanted to find out whether she had also been subjected to female genital mutilation. Several women who presented with a history of/previous type 3 said they had been partially ‘opened’ by their husband. Figure 4 demonstrates the type of female genital mutilation by number of women who attended each year.
Women presented with a multitude of uro-gynaecological symptoms (Table 6). The most common were dysuria, dyspareunia/apareunia, dysmenorrhea or recurrent infections. Those with type 3 experienced the most problems and usually experienced all four symptoms. Several women with history of/previous type 3 presented with continuing uro-gynaecological issues, despite having been deinfibulated, and more than 30 women were found to have fused anterior scar tissue and could only be partially deinfibulated. In a few cases, where the labia majora had been cut and stitched, the clitoral glans, labia minora and prepuce were found to be fully intact beneath the scar. There were also cases of labial elongation, tattooing and two women with anal-vaginal fistulas.
Table 6. Uro-gynaecological symptoms reported
| Symptom | Type | Tota | |||
|---|---|---|---|---|---|
| I | II | III | History of/previous type III | ||
| Dysuria | 1 | 6 | 91 | 13 | 111 |
| Dyspareunia or apareunia | 7 | 28 | 180 | 18 | 234 |
| Dysmenorrhea | 2 | 4 | 246 | 14 | 268 |
| Recurrent infections | 2 | 6 | 95 | 15 | 119 |
For many women, penetrative sexual intercourse was not possible before deinfibulation, as the diameter of the introitus was less than 1cm. Several women described enduring years of painful, forced vaginal intercourse resulting in bleeding and perineal damage and a few disclosed experiencing anal intercourse. Often women reported being given repeated antibiotic prescriptions for recurrent urinary tract infections by their GP. Other recorded symptoms included: clitoral or vulval pain, being unable to tolerate cervical smears, urinary incontinence, prolapse, lack of sexual pleasure, recurrent clitoral abscesses and cysts, and third and fourth degree tears during childbirth. Several women had been reinfibulated repeatedly during childbirth, some as many as six or seven times, in countries such as Somalia, Sudan and Saudi Arabia.
Therapeutic variables
Of the 526 women who had type 3 female genital mutilation, the primary reason they attended the service (452/526; 85.9%) was for deinfibulation under local anaesthetic (Table 7). This was performed by specialist midwives (or trainee doctors or midwives under their supervision). Some women attended a first appointment prior to deinfibulation while others (often if travelling from outside London) chose to be deinfibulated on the same day as walk-in cases. Over half were about to get married or had just been married.
Table 7. Therapeutic interventions
| Management | Frequency, n=808 (%) |
|---|---|
| Deinfibulation under local anaesthetic | 452 (55.9) |
| Referred for deinfibulation under general anaesthetic | 22 (2.7) |
| Uro-gynaecology referral | 134 (16.6) |
| Women had at least one counselling session | 90 (11.1) |
| Not recorded/other management | 68 (8.4) |
| Report for Home Office asylum application | 44 (5.4) |
| Woman wanted to know what type of female genital mutilation she has | 32 (4.0) |
| Women DNA deinfibulation appointment | 17 (2.1) |
In one case, a woman experienced extreme pain post-procedure, caused by an exposed nerve ending, and required further surgery by a consultant uro-gynaecologist. This was the only serious reported complication since opening in 2008. Women rarely required antibiotics for post-deinfibulation infection, and emergency intervention during the procedure was never required.
Many attendees required more than one intervention. Almost all of the 44 women requesting clinical documentation to support their asylum application required a uro-gynaecology referral and/or wanted counselling, and more than one third of this group were Nigerian. Other asylum reports were for women from Egypt, Eritrea, Gambia, Guinea, Iraq, Kenya, Senegal, Sierra Leone and Sudan.
Recording psychological symptoms began from 2015 (Table 8). The majority (59.6%) of women who attended reported at least one, and often a combination of, symptoms including depression, post-traumatic stress disorder, flashbacks and nightmares, with 129 women taking up at least one counselling session.
Table 8. Most common psychological symptoms recorded from 2015–2019
| Symptom | Frequency, n=808 (%) | ||||
|---|---|---|---|---|---|
| 2015 | 2016 | 2017 | 2018 | 2019 | |
| Depression or post-traumatic stress disorder | 23 (2.8) | 11 (1.4) | 19 (2.4 | 32 (4.0) | 44 (5.4 |
| Flashbacks or nightmares | 10 (1.2) | 5 (0.6) | 5 (0.6) | 3 (0.4) | 16 (2.0 |
The average length of time from making contact to first appointment was two weeks. Consultations lasted on average 30 minutes to one hour, and longer appointments of approximately 1.5 hour were allocated for deinfibulations. Referrals to the link consultant for fast track deinfibulation under general anaesthetic were chosen/recommended for women with particularly traumatic memories, those suffering flashbacks or touch/needle phobia or with a complex presentation (eg, epidermoid inclusion cyst). Surgery was usually performed within 4–6 weeks of referral.
Safeguarding
Three adult social care referrals, (all for domestic violence concerns) and nine referrals to children's social care were made. Three women disclosed that younger sisters, under 18 years old had female genital mutilation, and six mothers disclosed that their daughters, aged under 18 years, had female genital mutilation. Overall, there were three mandatory reporting duty referrals (for those cases reported after the 2015 legislation was introduced) and two female genital mutilation protection orders were sought.
In 2011 two messages were left on the clinic answer machine from a man requesting female genital mutilation for his daughters. We informed the local child abuse investigation team who were able to trace the family. The man was arrested and the daughters were temporarily placed into care. We also received one threatening letter and two threatening phone calls.
On occasion women disclosed rape, forced early marriage, domestic violence and abuse linked to faith or belief. Several women had been trafficked and/or subjected to modern slavery. Women from West Africa were more likely to have suffered other intersectional gender-based violence in addition to female genital mutilation, and many reported being under pressure from families ‘back home’ to continue the practice.
Most women were adamant they would never subject their daughters to female genital mutilation having recalled traumatic cutting experiences and suffering the health consequences of female genital mutilation. They frequently said that female genital mutilation was practised for cultural reasons or tradition, but other justifications were mentioned. For example to ‘prevent women from being promiscuous’ or stop the ‘clitoris growing until it reaches the floor’. Women often referred to type 3 as ‘pharaonic’ and used the word ‘sunna’ to describe a less severe type of female genital mutilation, implying some form of religious obligation. Furthermore, despite using the phrase sunna, women rarely said female genital mutilation was required by their religion. Although the majority of clinic attendees were Muslim, we saw women from other faiths, such as Coptic Christians from Egypt and other Christian-based faiths from Ethiopia and Nigeria.
Discussion
The data from this study illustrate that female genital mutilation is still a significant problem for non-pregnant women living in the UK. Variations in attendance to the specialist clinic over the last 11 years may reflect changes in legislation, societal awareness and local advertising, but attendance averaged at 72 new appointments per year. In recent years, there has been an increase in referrals from healthcare professionals and charities/non-governmental organisations, as well as increased ethnic diversity, more women with type 1 and 2 female genital mutilation and more requests for asylum reports and counselling. Notably, the number of requests for deinfibulation under local anaesthetic have remained consistent. Nearly half of women who requested deinfibulation in 2019 were in the 18–25 year age range, demonstrating that type 3 female genital mutilation is still prevalent, despite education and international attempts to stop the practice over the last 30 years.
The profiles of women attending the clinic were extremely varied, reflecting the fact that there is no one homogenous female genital mutilation practising community. Women's ages ranged from 18 years to post-menopausal, with some experiencing symptoms for more than 40 years (Karlsen et al, 2019). Some women were highly educated, multilingual professionals while others spoke basic or no English. In particular, the number of healthcare professionals and carers accessing the service was striking (Karlsen et al, 2019).
These findings corroborate previous research acknowledging the silence surrounding female genital mutilation (Dixon et al, 2018; Rittenberg, 2018; Evans et al, 2019). Some women specifically asked to not see the Somali health advocate, as they preferred to remain completely anonymous and were fearful of female genital mutilation community members discovering that they had attended the service. Some women also reported community pressure to remain ‘closed’ prior to marriage.
Worryingly, a small but growing body of evidence demonstrates that introduction of the 2015 Serious Crime Act legislation (Gov.uk, 2015) and enhanced dataset collection (NHS Digital, 2020) may have resulted in women being fearful of presenting to female genital mutilation services (Mathers and Rymer, 2015; Dixon et al, 2018; Evans et al, 2019; Karlsen et al, 2019). However, the number of women who said that female genital mutilation took place while they were on holiday reinforces the relevance of the Serious Crime Act, which legislates that parents can be prosecuted for failing to protect their daughters from being cut by extended family/community members (Gov.uk, 2015).
Clinical issues
The present study's data are consistent with WHO (2020) evidence that type 3 female genital mutilation is mostly practiced in the northeast region of Africa, corresponding with high prevalence of Somali, Sudanese and Eritrean communities in West London. In the present study's sample, 71% of Somali women were cut between age 5 and 10 years old, which correlates closely with UNICEF's (2020) country profile, reporting 82% of Somali women experienced female genital mutilation between the ages of 5 and 9 years.
The burden of symptoms experienced by women attending the clinic is consistent with that reported in other studies (Momoh et al, 2001; Gordon et al, 2007; Elneil, 2016; Albert and Wells, 2020; Hanlon and Hex, 2021; UNICEF, 2022). However, this may be an underestimation, as recent research from Norway highlighted the complex factors involved for women to recognise that their symptoms are caused by female genital mutilation rather than believing them to be a ‘normal’ consequence of womanhood (Ziyada and Johansen, 2021). Furthermore, the present study's data showed that many women with fused anterior scar tissue found that, even after deinfibulation, the introitus remained impenetrable for comfortable sexual intercourse. This is rarely discussed in any female genital mutilation literature but warrants further investigation (Albert and Wells, 2020).
The incidence of psychological symptoms, identified by previous research (Okonofua et al, 2002; Essén and Johnsdottir, 2004), confirms the need for counselling provision in female genital mutilation clinics (NHS England, 2019a). Women disclosed difficulties experiencing sexual pleasure, complained of not feeling ‘whole’ and, in recent years, increasingly requested clitoral and/or labial reconstruction. Previous UK care for women with female genital mutilation has focused on deinfibulation to prepare for childbirth and safeguarding assessments. There are few clinics that offer psycho-sexual support or long-term counselling and there are no reconstruction services. Women spoke of their knowledge of reconstruction via social media, and some had either already had reconstruction or made plans to seek this surgery in other countries, including Germany, France or Kenya.
The present study's data show that the uptake of one-to-one counselling increased substantially after 2015, correlating with an increase in attendees from non-Somali ethnic backgrounds. This may be because of a reluctance to seek counselling within the Somali community or may be an indication that women who have suffered female genital mutilation with additional intersectional violence are more likely to seek this service. This requires further exploration.
The majority of deinfibulations were performed under local anaesthetic as women often said they were scared of ‘having a needle in their back’. Gordon et al (2007) reported that 90% of patients preferred the procedure under general or epidural anaesthetic; however, the experiences from the Sunflower Clinic concurs with those of other UK services (Momoh et al, 2001; Sosa, 2004; Paliwal et al, 2014). Over the 11-year period, only 22 women chose deinfibulation under general anaesthetic. One case, out of 452 deinfibulations, required an acute intervention the next day by a consultant gynaecologist. This suggests that simple deinfibulation under local anaesthetic in an outpatient or community setting is safe when performed by trained expert midwives.
Many women travelled a long way to access the service. In 2019, the Acton clinic model became the prototype on which NHS England (2019b) based its new national female genital mutilation support clinics (Albert and Wells, 2020). These clinics, located in areas of high prevalence of female genital mutilation practising communities, should mean that women do not have to travel as far to access holistic multidisciplinary care.
The implications of deinfibulation for later pregnancy and childbirth are not known. A number of women present every year to the pregnant women's service who were deinfibulated at the clinic prior to conception. No data capture how many of these nulliparous women go on to have a successful vaginal birth after deinfibulation. A longitudinal prospective study is needed to examine long-term outcomes of deinfibulation and, in particular, childbirth outcomes in this population.
Several parous women with type 3 described receiving a medio-lateral or bilateral episiotomy during childbirth (rather than an anterior incision to deinfibulate them). These cut edges were then sutured together afterwards leaving them with intact type 3 female genital mutilation. It is not known whether this persists in maternity units in the UK or whether improvements in the education of healthcare professionals have stopped this practice.
Limitations
Some data were missing or unretrievable from records prior to the relocation of the clinic. The methodology of a retrospective case note review means that it was not possible to establish cause and effect relationships.
Recommendations
The success of the Somali satellite television advertisement and the increasing use of modern media to make contact with clinic staff indicate that specialist services could use innovative methods to publicise clinics. Research is required to investigate whether women would accept and benefit from being asked about female genital mutilation during routine gynaecology review (in settings such as sexual health/family planning/genitourinary medicine clinics/gynaecology appointments/emergency departments etc), and GP surgery new patient registrations. There are currently campaigners lobbying for this to become mandatory.
The high uptake of counselling demonstrates this could benefit women if available in all female genital mutilation clinics (including those located in maternity units). Sensitive safeguarding discussions and trauma-informed conversations around anatomy and physiology, sexual pleasure and education about the health consequences of female genital mutilation require further investigation. This will help to inform how ideas of bodily integrity and negative cultural stereotypes affect women who have suffered female genital mutilation and may serve to support behaviour change and prevent female genital mutilation in the future.
Conclusions
This article demonstrates that female genital mutilation specialist clinics (such as the one described) provide a service that is not available in the mainstream UK health system. Despite worldwide attempts to eliminate female genital mutilation, the data suggest that there remain a significant number of women with female genital mutilation in the UK, including many with type 3 from a diverse age range.
Clinical care has evolved as more is understood about women's individual needs and as the profile of clients diversifies. Only one post-deinfibulation clinical complication required consultant gynaecological intervention, suggesting that this midwife-led service model is cost effective, safe and acceptable.
Consistent attendance figures, women being recommended by family or friends and positive feedback, all suggest a degree of service satisfaction. However, it is not known whether more women want/need help but do not know how to access it or, perhaps, even recognise they need help. The impact of policy and legislation introduced in 2015 has never been formally evaluated and it is unknown whether women may be too scared or ashamed to present to health services for fear of recrimination.
Key points
- Specialist female genital mutilation clinics for non-pregnant women remain an important component of NHS care.
- This retrospective case note review examined referral patterns, clinical findings and interventions over 11 years at a UK specialist clinic for non-pregnant women with female genital mutilation.
- More than 2000 consultations were conducted; two thirds of women had type 3 mutilation and interventions included deinfibulation under local anaesthetic (many as same day walk-in cases), clinical reports for asylum applications and trauma counselling.
- Women with type 3 female genital mutilation need access to deinfibulation.
- Midwife-led services are cost effective, safe and acceptable to clients.
CPD reflective questions
- Has policy and legislation introduced in the 2015 Serious Crime Act had an impact on access to female genital mutilation specialist services?
- What innovative means could be used to advertise specialist services?
- Should women be asked about female genital mutilation during routine gynaecology consultations or during GP appointments?